全身性エリテマトーデス
Systemic lupus erythematosus
2016年6月16日 Nature Reviews Disease Primers Article number: 16039 (2016) doi: 10.1038/nrdp.2016.39
全身性エリテマトーデス(SLE)は、皮膚、関節、中枢神経系および腎臓など、多くの臓器が障害される自己免疫疾患である。通常、SLEは特定人種の出産適齢期の女性に好発する。希少遺伝性の単一遺伝子補体欠損症とSLEに強力な関連があるものの、大多数のSLE患者で多遺伝子性遺伝が認められる。遺伝と環境因子(特にUV線曝露、EBウイルス感染およびホルモン性因子)の相互作用によってSLEが発症すると、サイトカイン、T細胞、B細胞およびマクロファージレベルでの免疫不全状態が生じる。SLEの診断は主に臨床所見に基づいて行われるが、症状が多様であることが問題になっている。分類基準は臨床試験の役には立ったが、この60年間にSLEの適応が認可された薬剤はベリムマブただ1つである。10年死亡率は改善し、シクロホスファミドやグルココルチコイドなど古典的薬剤による毒性的有害作用の問題は、ミコフェノール酸モフェチルやグルココルチコイド節約型レジメンなどの新しい薬剤によって一部克服されている。しかし、今以上の改善は腎障害や神経精神障害による有害作用と診断の遅れによって阻まれている。このような負担のみならず、SLEでは早発性心血管疾患の発症リスクが増加することに加え、免疫抑制療法により感染リスクも増加する。今後の課題として、治療抵抗例や疲労などの症状が挙げられる。将来、新たな治療法による転帰の改善が期待されるとともに、幹細胞の改良や遺伝子工学により治癒への道が開ける可能性がある。
PrimeView
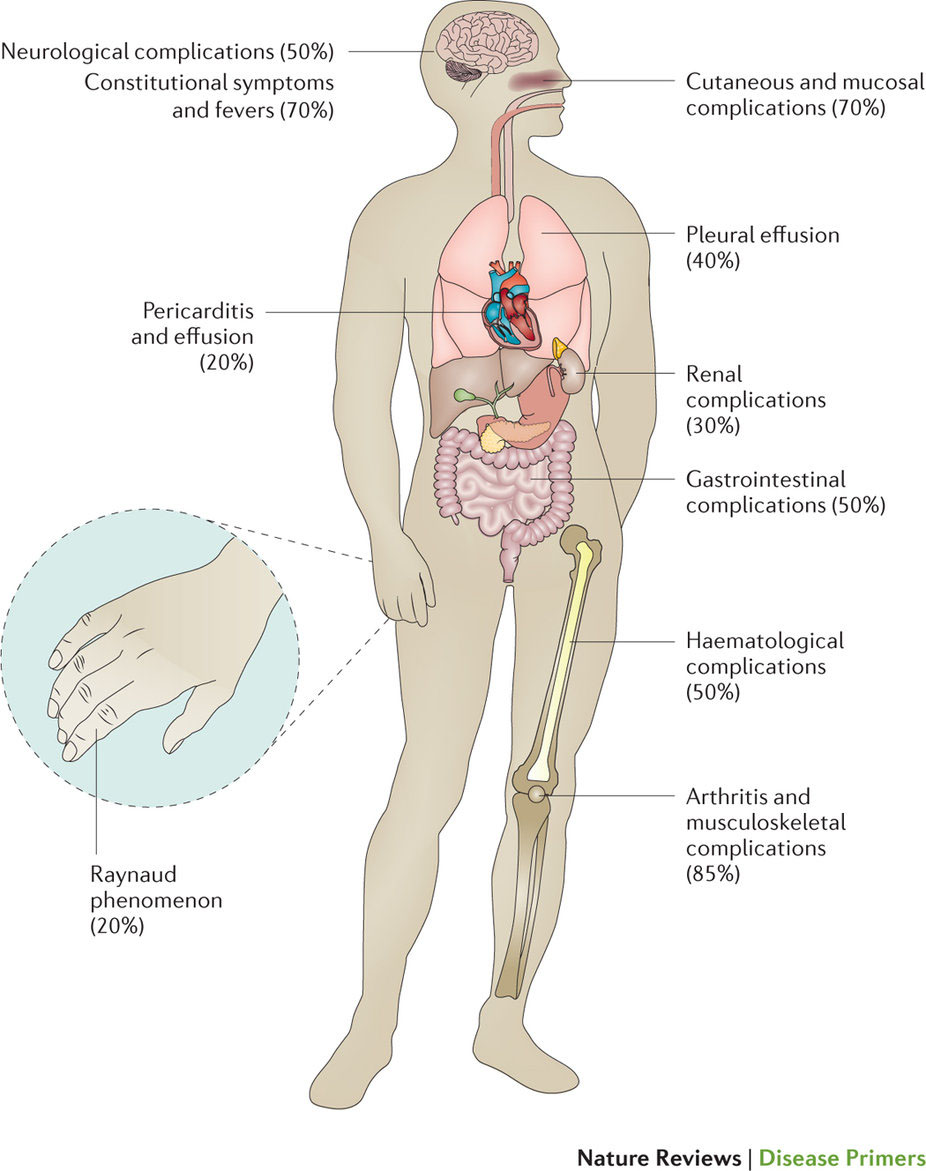
全身性エリテマトーデス(SLE)は、場合によっては致命的になる慢性自己免疫疾患である。このPrimeViewでは、非常に様々な臨床症状および重症度をもつSLEの多様性について取りまとめる。早期診断と再燃予防は、長期罹患率と死亡率を減少させる上で重要である。
本Primerの図解サマリー