肝硬変における慢性肝不全の急性増悪
Acute-on-chronic liver failure in cirrhosis
2016年6月9日 Nature Reviews Disease Primers Article number: 16041 (2016) doi: 10.1038/nrdp.2016.41
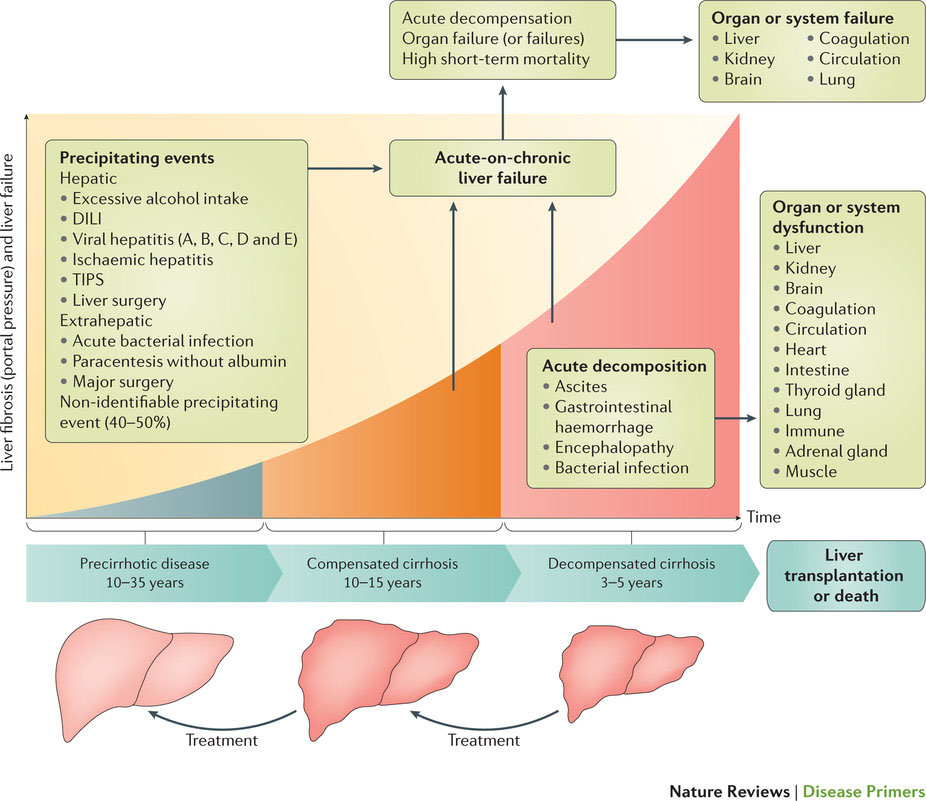
慢性肝不全の急性増悪(ACLF)の定義には議論がある。欧州および北米では、欧州肝臓学会/慢性肝不全(ESAL-CLIF)コンソーシアムのガイドラインに従ってこの用語を取り扱っている。ここでのACLFの定義は、肝硬変患者に発症する症候群の1つで、急性代償不全、臓器不全および高い短期死亡率を特徴とする病態とされている。急性代償不全で入院した患者の1/3は、ACLFを呈しているか、あるいは入院中にこの症候群を発症する。ACLFは、細菌感染症、急性アルコール性肝炎、薬剤性肝炎またはウイルス性肝炎などの引き金となる事象との密接な時間的関係において頻発する。しかし、患者の約40%については引き金となる事象が特定できていない。ACLFの発症機構には、感染症や急性肝障害による全身性炎症が関与しているが、引き金となる事象が特定できない症例では、おそらく、細菌または細菌産生物の腸内局在変化が関係するとみられる。ACLFのグレードは臓器不全の数に応じて3段階(ACLFグレード1—3)に分けられ、グレードが高いほど死亡率が高い。最も多く見られる臓器不全は肝臓と腎臓の不全であり、血液凝固、脳、循環器系および呼吸器系の不全がそれに続く。ACLFに関連する28日死亡率は30%である。標準治療で回復するのは、ACLFのグレードに応じて、患者の16—51%のみであり、ACLFが安定または進行した患者の割合は今も多いままである。ACLFグレード2および3の特定患者に肝移植を行うことで、6ヵ月生存率が10%から80%に上昇する。
PrimeView
このPrimeViewでは、肝硬変における慢性肝不全の急性増悪の病態生理について取りまとめる。肝硬変患者では、敗血症やアルコール性肝炎などの炎症が引き金となって急性肝代償不全と臓器不全が生じることがあり、そのため短期死亡率が高くなる。
本Primerの図解サマリー