肝細胞がん
Hepatocellular carcinoma
2016年4月14日 Nature Reviews Disease Primers Article number: 16018 (2016) doi: 10.1038/nrdp.2016.18
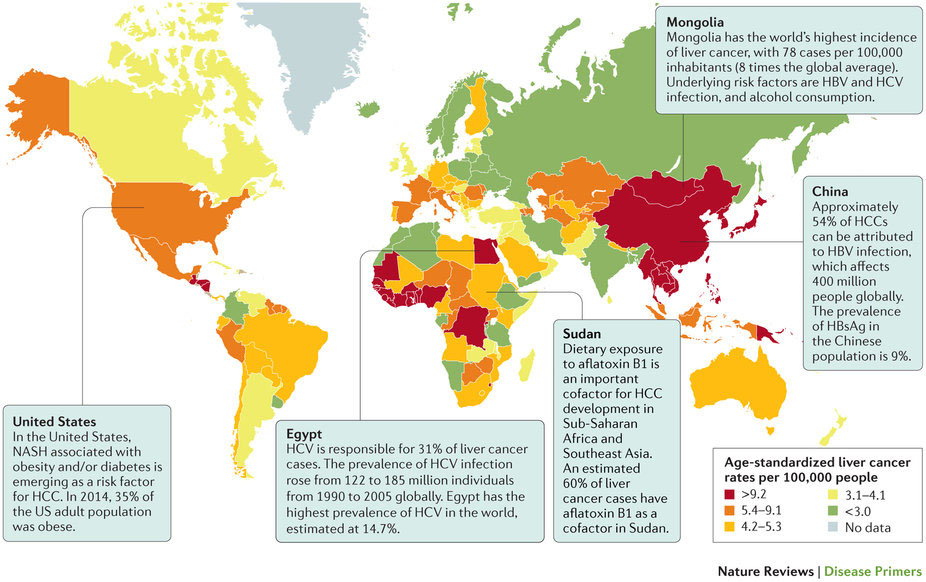
肝臓がんは世界のがん関連死亡原因の第2位であり、毎年約85万人が新たに発症する。原発性肝臓がんの約90%は肝細胞がん(HCC)が占めている。HCCの主な発症リスク因子には、B型およびC型肝炎ウイルス感染、アルコール摂取、真菌代謝物であるアフラトキシンB 1暴露などがあり、いずれもよく知られている。非アルコール性脂肪性肝炎などの新しいリスク因子も浮上している。HCCの分子病態生理への理解が深まったことで重要なドライバー遺伝子変異の同定が進んだが、最も多く見られる変異の分子標的薬の開発には至っていない。HCCの分子分類はまだ確立されておらず、現在の臨床アルゴリズムではBarcelona Clinic Liver Cancer病期分類が中心に位置づけられており、予後予測に基づく患者の層別化とそれに応じた治療法が推奨されている。サーベイランスプログラムによって早期がんの発見が可能になった。早期がんは、肝切除、肝移植または局所焼灼療法のような根治的治療に適している。病期が進展したがんの場合、生存率における有益性が確認されているのは化学塞栓療法(中間期HCC向け)とソラフェニブ治療(進行HCC向け)だけである。HCCの管理法における主なアンメットニーズへの取り組みとして、術後療法ならびに中間期と進行期のがんに対する新しい治療法の発見とそれらの併用が進められるだろう。さらに、治療層別化のバイオマーカー、ドライバー遺伝子変異の標的化またはシグナルカスケードの活性化あるいはその両方による個別化治療、ならびにQOLの有効な測定法も必要となろう。最近行われた中間期と進行期のがんに対する全身化学療法の評価では、試験デザインの改良と新しい治療法の定義の必要性が指摘されている。
PrimeView
肝細胞がん(HCC)の主な発症リスク因子には、肝硬変、アルコールの過剰摂取、ウイルス性肝炎などがある。このPrimeViewでは唯一の全身治療および現在のフロントライン治療である肝移植によるHCCの管理について取りまとめる。
本Primerの図解サマリー