脳動静脈奇形
Brain arteriovenous malformations
2015年5月28日 Nature Reviews Disease Primers Article number: 15008 (2015) doi: 10.1038/nrdp.2015.8
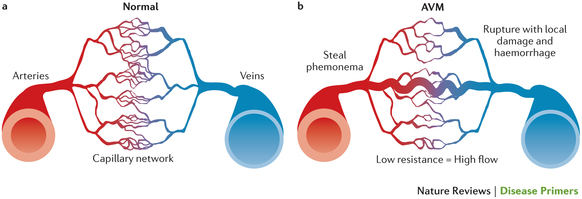
動静脈奇形には、栄養動脈と流出静脈の異形成血管が絡み合った塊(ナイダス)が見られる。動脈と静脈の間に毛細血管がないため、血管吻合部の血流が速くなり抵抗性が低くなる。脳の動静脈奇形は、有病率が低いと推測されているものの、若年成人における脳出血の主な原因になっている。未破裂の動静脈奇形の年間出血率は1%程度である。1度破裂すると、関連動脈瘤、深部局在、深部静脈への流出および加齢に応じて再発リスクが5倍に上昇する。動静脈奇形は、長い間先天性疾患と考えられてきたが、新しい動物モデルと遺伝子研究による最近の結果から、傷害後の脈管形成異常、遺伝子変異および/または血管新生によっても生じることが示唆された。動静脈奇形の表現型の特徴には年齢による違いがあり、小児では瘻孔性病変が見られるのに対し、成人では奇形性病変が見られる。主にCT、MRIおよび血管撮影法などの画像検査によって診断が行われる。動静脈奇形の管理は、経過観察、顕微鏡下切除術、血管内塞栓術および定位放射線治療、またはこれらの組み合わせによって行われる。未破裂の動静脈奇形の管理について合意された方法はないが、最近の研究から、追跡期間の短い介入療法よりも医療管理の方が患者に良い結果をもたらすことが示されている。対照的に、破裂した動静脈奇形の再出血予防には介入療法が望ましい。新しい発症機序の発見によって、管理方法は進化し続けている。また、信頼できる動物モデルによって、動静脈奇形の形成を予防し、血管を閉塞および/または強化して破裂リスクを低下するような薬剤が開発される可能性が高まっている。