慢性膵炎
Chronic pancreatitis
2017年9月7日 Nature Reviews Disease Primers Article number: 17060 (2017) doi: 10.1038/nrdp.2017.60
慢性膵炎は、膵実質障害またはストレスに対する持続的病理学的反応を起こす遺伝的素因や環境因子を含むさまざまなリスク因子を有するヒトの膵臓の病理学的線維性炎症性症候群として定義される。潜在的原因としては、毒性因子(アルコール摂取、喫煙など)、代謝異常、遺伝的素因、自己免疫反応、閉塞機序などが挙げられ、特発性の発症機構も存在する。慢性膵炎の病態生理学はかなり複雑であり、腺房細胞障害、腺房のストレス反応、膵管機能不全、炎症の持続または悪化、あるいは神経免疫のクロストークなどの関与が考えられるが、これらの発症機構は完全には解明されていない。慢性膵炎は、膵臓での炎症の進行を特徴とし、膵萎縮あるいは組織の線維化によって内分泌組織と外分泌組織に進行性障害が現れる。その結果、反復性腹痛や持続性腹痛、糖尿病(内分泌不全)および消化不良(外分泌不全)などを認めるようになる。所見の変化がわずかで不明瞭な上に、他の疾患とも重なるため、早期慢性膵炎の診断は難しいといわれている。しかし、病態が進行すると、膵実質での不規則な線維化や石灰化をはじめ、膵管の拡張、歪曲および狭窄、仮性嚢胞、胆嚢内胆管狭窄、十二指腸の狭窄、上腸間膜動脈血栓症、門脈血栓症、脾静脈血栓症などの特徴的所見が現れる。治療では、薬物治療、放射線治療、内視鏡的治療、外科手術などが行われるが、エビデンスに基づいた治療法は限られている。このPrimerでは、慢性膵炎の病態生理学、症状、有病率、管理法および合併症に関する理解が大いに進展した点について解説する。
PrimeView
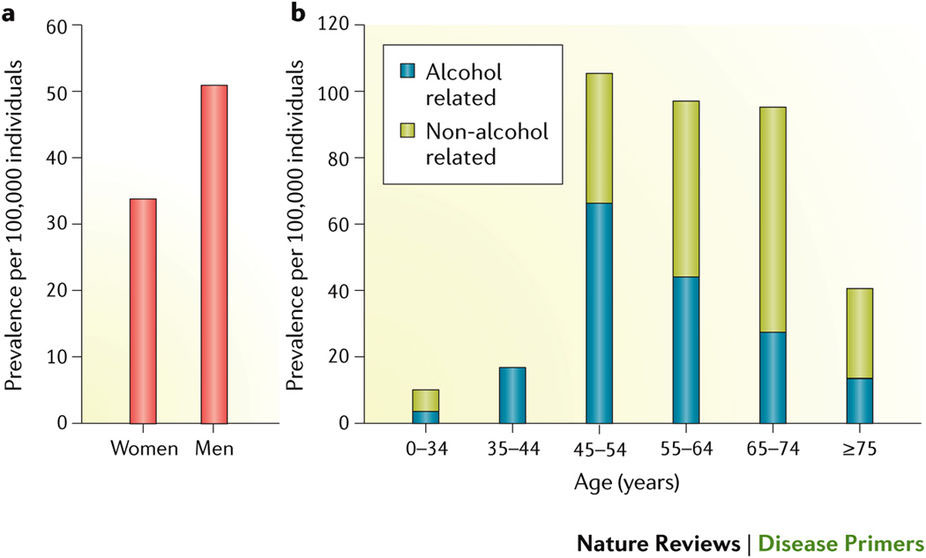
慢性膵炎は過度のアルコール摂取が原因であることが多く、喫煙はこれとは独立したリスク因子である。これら以外にも、遺伝的素因、代謝障害、慢性閉塞性の原因(結石など)、自己免疫などの原因をはじめ特発性の慢性膵炎も存在する。
本Primerの図解サマリー
Chronic pancreatitis is defined as a pathological fibro-inflammatory syndrome of the pancreas in individuals with genetic, environmental and/or other risk factors who develop persistent pathological responses to parenchymal injury or stress. Potential causes can include toxic factors (such as alcohol or smoking), metabolic abnormalities, idiopathic mechanisms, genetics, autoimmune responses and obstructive mechanisms. The pathophysiology of chronic pancreatitis is fairly complex and includes acinar cell injury, acinar stress responses, duct dysfunction, persistent or altered inflammation, and/or neuro-immune crosstalk, but these mechanisms are not completely understood. Chronic pancreatitis is characterized by ongoing inflammation of the pancreas that results in progressive loss of the endocrine and exocrine compartment owing to atrophy and/or replacement with fibrotic tissue. Functional consequences include recurrent or constant abdominal pain, diabetes mellitus (endocrine insufficiency) and maldigestion (exocrine insufficiency). Diagnosing early-stage chronic pancreatitis is challenging as changes are subtle, ill-defined and overlap those of other disorders. Later stages are characterized by variable fibrosis and calcification of the pancreatic parenchyma; dilatation, distortion and stricturing of the pancreatic ducts; pseudocysts; intrapancreatic bile duct stricturing; narrowing of the duodenum; and superior mesenteric, portal and/or splenic vein thrombosis. Treatment options comprise medical, radiological, endoscopic and surgical interventions, but evidence-based approaches are limited. This Primer highlights the major progress that has been made in understanding the pathophysiology, presentation, prevalence and management of chronic pancreatitis and its complications.