発作性夜間ヘモグロビン尿症
Paroxysmal nocturnal haemoglobinuria
2017年5月18日 Nature Reviews Disease Primers Article number: 17028 (2017) doi: 10.1038/nrdp.2017.28
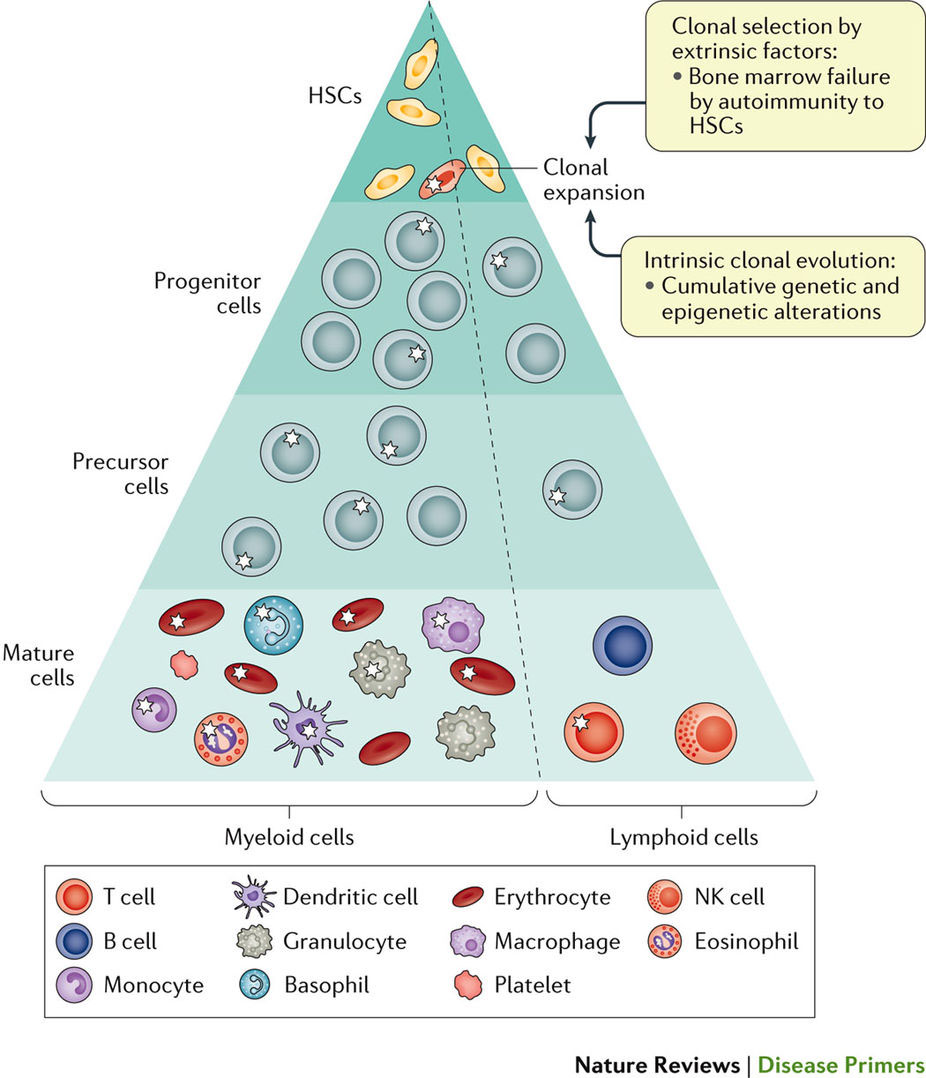
発作性夜間ヘモグロビン尿症(PNH)は慢性造血幹細胞(HSC)疾患であり、骨髄不全をはじめ、溶血性貧血、血栓症、平滑筋ジストニアなどを認めることがある。PNHは、ホスファチジルイノシトールN-アセチルグルコサミニルトランスフェラーゼのサブユニットAの遺伝子であるPIGAの体細胞変異に起因するHSCの単クローン性または多クローン性疾患である。PIGAの遺伝子産物はグリコシルホスファチジルイノシトール(GPI)アンカーの生合成に必要とされる。そのため、PIGAに変異が生じると、補体崩壊促進因子(別名:CD55)やCD59糖タンパク質(CD59)などの補体阻害因子として作用するGPIアンカータンパク質が欠損する。PNHの臨床症状は、PIGAの体細胞変異を保有するHSCクローンが増殖優位性を獲得して分化するときに発現し、GPIアンカータンパク質を欠損した成熟血球が産生される。CD55およびCD59が欠損した赤血球は血管内溶血を起こしやすくなるため、血栓症につながるだけでなく、PNHの罹患率と死亡率の主要な原因になっている。補体活性化により生じるアナフィラトキシン(C5aなど)の蓄積も役割を担うと考えられている。PNHの自然経過は非常に多様であり、寛解することもあれば生命が脅かされることもある。治療には、終末補体阻害薬の使用や骨髄移植が行われる。現在、認可されているPNH治療薬はモノクローナル抗体のエクリズマブだけであり、補体阻害作用を介して高い効果を発揮することが明らかにされている。
PrimeView
造血幹細胞のPIGAに体細胞変異が起こることで、グリコシルホスファチジルイノシトールアンカータンパク質を欠損した赤血球が産生される。このような赤血球は補体活性化により溶血を起こしやすくなるため、発作性夜間ヘモグロビン尿症が発症する。このPrimeViewでは発作性夜間ヘモグロビン尿症の複雑な発症機構について図解する。
本Primerの図解サマリー
Paroxysmal nocturnal haemoglobinuria (PNH) is a clonal haematopoietic stem cell (HSC) disease that presents with haemolytic anaemia, thrombosis and smooth muscle dystonias, as well as bone marrow failure in some cases. PNH is caused by somatic mutations in PIGA (which encodes phosphatidylinositol N-acetylglucosaminyltransferase subunit A) in one or more HSC clones. The gene product of PIGAis required for the biosynthesis of glycosylphosphatidylinositol (GPI) anchors; thus, PIGA mutations lead to a deficiency of GPI-anchored proteins, such as complement decay-accelerating factor (also known as CD55) and CD59 glycoprotein (CD59), which are both complement inhibitors. Clinical manifestations of PNH occur when a HSC clone carrying somatic PIGAmutations acquires a growth advantage and differentiates, generating mature blood cells that are deficient of GPI-anchored proteins. The loss of CD55 and CD59 renders PNH erythrocytes susceptible to intravascular haemolysis, which can lead to thrombosis and to much of the morbidity and mortality of PNH. The accumulation of anaphylatoxins (such as C5a) from complement activation might also have a role. The natural history of PNH is highly variable, ranging from quiescent to life-threatening. Therapeutic strategies include terminal complement blockade and bone marrow transplantation. Eculizumab, a monoclonal antibody complement inhibitor, is highly effective and the only licensed therapy for PNH.