くる病
Rickets
2017年12月21日 Nature Reviews Disease Primers 3 : 17101 doi: 10.1038/nrdp.2017.101
くる病は、カルシウムとリンの血中濃度の低下によって起こる骨疾患の1つである。臨床症状は、発症年齢と病因によって異なるが、下脚の弓状変形、低身長、関節の拡大などが現れる。くる病の原因は栄養欠乏だけでなく遺伝子異常も関係すると考えられており、現在までに、ビタミンDの代謝または作用、線維芽細胞増殖因子23(FGF23)の産生と分解、腎臓のリン排泄能、骨代謝などに関与するタンパク質の遺伝子の変異が報告されている。栄養性くる病の罹患率は200年前と比べて大幅に減少したが、最近、いくつかの先進国で再び増加し始めている。とりわけ、浅黒い肌を持つ未熟児や母乳幼児では発症リスクが高い。通常、診断は、病歴、身体検査、生化学検査およびX線画像検査で行われる。栄養性くる病に限っては予防が可能とされており、カルシウムとビタミンDのサプリメントや栄養強化食品を摂取するか、日光浴との併用が行われる。典型的な栄養性くる病の治療では、カルシウムまたはビタミンD、あるいはその両方の補給が行われるが、まれにリンの補給が必要になることがある。ビタミンDの代謝または活性化の異常が原因で起こる遺伝性のくる病の管理では、活性型ビタミンDの投与が行われる。FGF23非依存性の低リン血症性くる病の治療では経口リン補給薬が使用されることが多いが、FGF23関連性くる病の通常治療では、リンと活性型ビタミンDが併用される。最近、抗FGF23抗体で有望な結果が示されたが、さらなる研究が必要である。
PrimeView
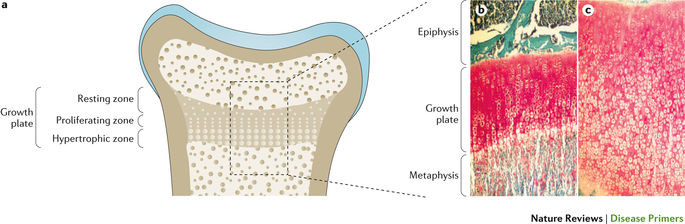
くる病は、カルシウムとリンの血中濃度の低下によって起こる骨疾患の1つで、主に、成長板の広がりとミネラル化不足につながる。くる病の罹患率は200年前と比べて大幅に減少したが、再び増加し始めている。
本Primerの図解サマリー
Rickets is a bone disease associated with abnormal serum calcium and phosphate levels. The clinical presentation is heterogeneous and depends on the age of onset and pathogenesis but includes bowing deformities of the legs, short stature and widening of joints. The disorder can be caused by nutritional deficiencies or genetic defects. Mutations in genes encoding proteins involved in vitamin D metabolism or action, fibroblast growth factor 23 (FGF23) production or degradation, renal phosphate handling or bone mineralization have been identified. The prevalence of nutritional rickets has substantially declined compared with the prevalence 200 years ago, but the condition has been re-emerging even in some well-resourced countries; prematurely born infants or breastfed infants who have dark skin types are particularly at risk. Diagnosis is usually established by medical history, physical examination, biochemical tests and radiography. Prevention is possible only for nutritional rickets and includes supplementation or food fortification with calcium and vitamin D either alone or in combination with sunlight exposure. Treatment of typical nutritional rickets includes calcium and/or vitamin D supplementation, although instances infrequently occur in which phosphate repletion may be necessary. Management of heritable types of rickets associated with defects in vitamin D metabolism or activation involves the administration of vitamin D metabolites. Oral phosphate supplementation is usually indicated for FGF23-independent phosphopenic rickets, whereas the conventional treatment of FGF23-dependent types of rickets includes a combination of phosphate and activated vitamin D; an anti-FGF23 antibody has shown promising results and is under further study.